
RESTECH ACQUIRES STRETTA® and SECCA®
April 24, 2018
Restech to Revisit the 47th Annual Symposium: Care of the Professional Voice
May 31, 2018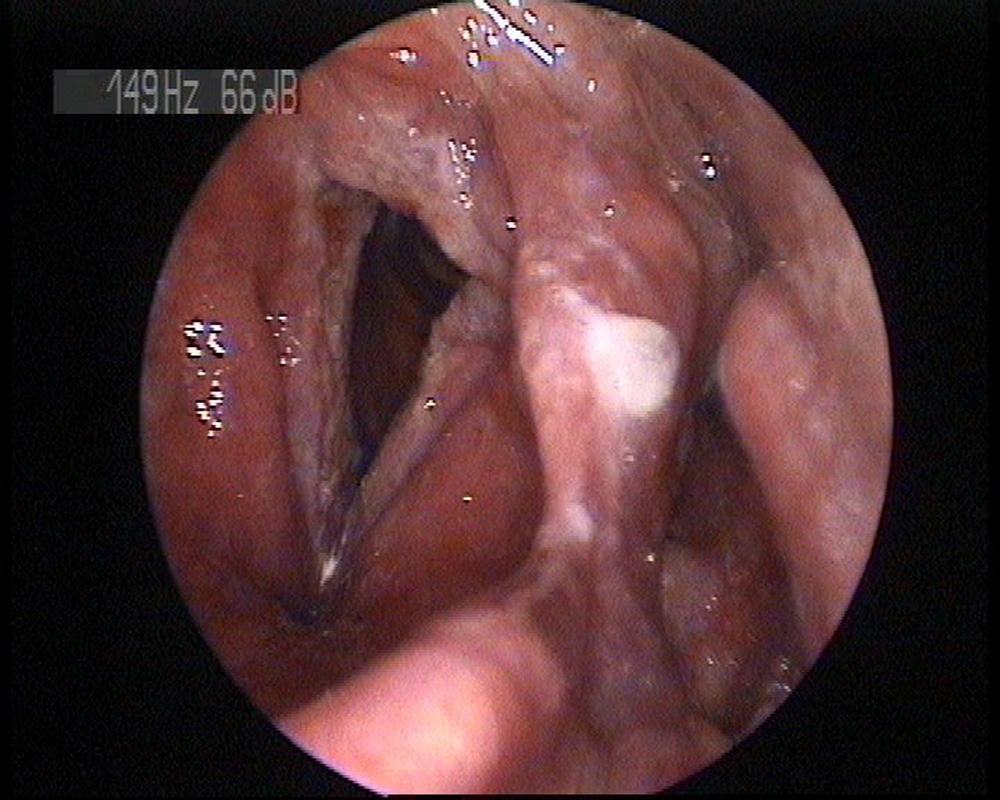
Dr. Josef Schlömicher-Thier
Chief of the International Voice Center Austria
Chief of the ENT Center in Neumarkt/Salzburg
Laryngology Specialist
CASE HISTORY & EVALUATION
A 60 year old male presented with hoarseness, a heavy cough, and voice problems extending back at least four years. Symptoms had recently exacerbated leaving the individual out of work on sick leave. The patient reported multiple prior pneumonias, but presented with a normal pulmonary exam at the time of the initial assessment.
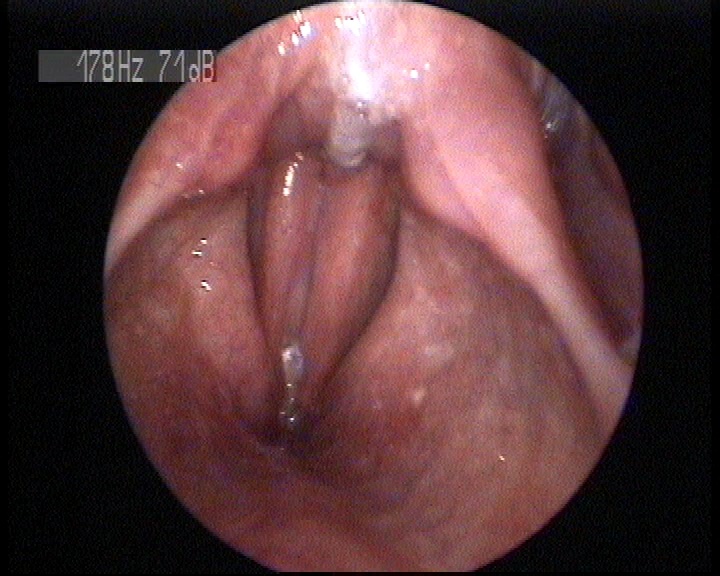
Prior to his office assessment, the patient was examined at a different hospital. This included the discovery of a minor hiatal hernia, which was accompanied by a negative esophageal manometry test and a negative duel channel pH test. Video Stroboscopy revealed hyperplasia/ leucoplakia. VRP showed a restricted mass.
Pre-Treatment Scores:
RSI=23 CSI=15 BSI=19 VHI=23
Pre-Treatment Images:
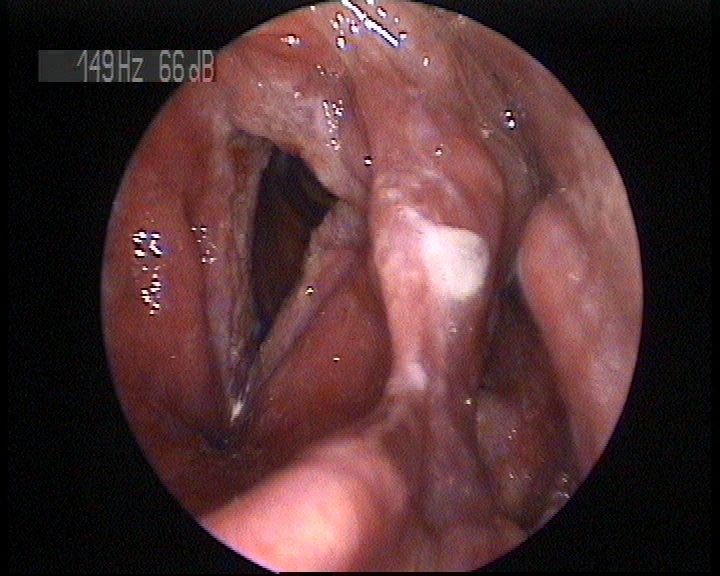
DIAGNOSIS
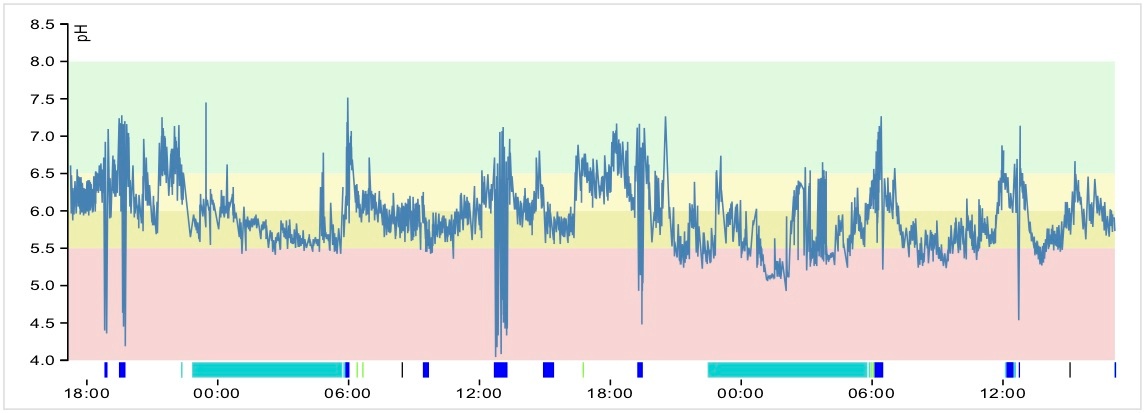
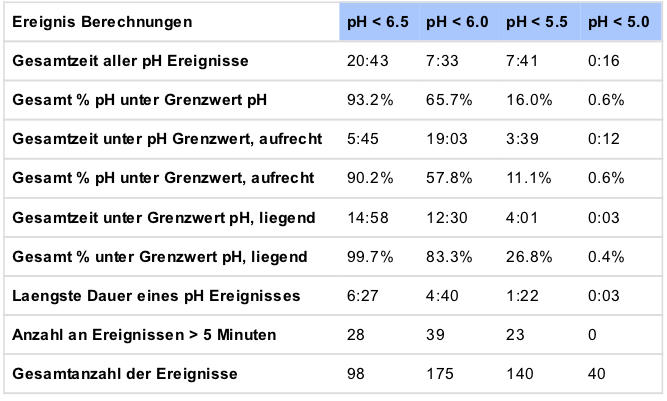
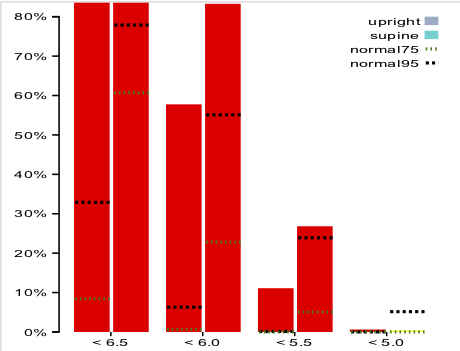
A 48 hour Restech pH Study showed a positive upright RYAN Score of 161.34. In addition, the patient exceeded the 95th percentile at the <5.5 threshold and the 75th percentile at the <5.0 threshold when supine. An esophageal Function TNE showed a clear hiatal hernia and reflux according to the LA Classification of two. The positive Restech test, coupled with the negative esophageal pH test and manometry provided a diagnosis of LPR.
Restech pharyngeal pH test results:
TREATMENT
A high dose PPI therapy of pantopracol (40mg BID) with Gaviscon and Antimycotica was initially prescribed. The hyperplasia reacted slowly however, so the treatment was changed to esemoptazol (40/20/40) with an evening H2 blocker for two weeks, reduced to 40mg BID step down and Lax Vox Therapy (8x4min per day) thereafter, which was very effective.
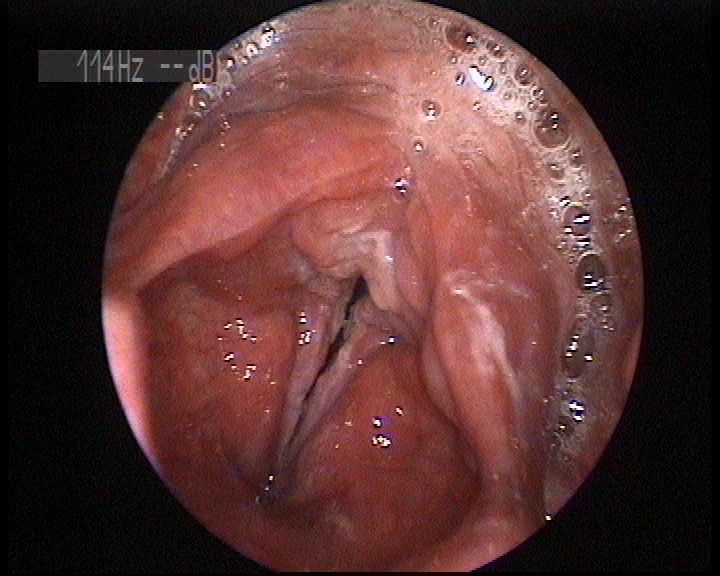
After three months all symptoms (notably the hyperplasia, cough, and vocal distress) had resolved and the medication was tapered to a halt. Ongoing lifestyle and dietary modifications were ordered along with a continued program of voice exercises (Lax Vox).
Post-Treatment Scores
RSI=4 CSI=6 BSI=7 VHI=8
OUTCOME AND CONCLUSION
Restech was essential to the diagnosis of LPR in this patient as the negative esophageal pH test and manometry had initially led the patient’s doctors to rule out reflux as the cause of his symptoms. The positive upright RYAN Score and Moderate to Severe Supine Acid Exposure Graph provided a critical insight into an appropriate treatment plan. This was further verified by the initial lack of progress on pantopracol. Ultimately, the patient’s symptom resolution provides a testament to the importance of a precise and individualized treatment plan.